EHR vs. EMR: What Health Care IT Actually Needs to Know About the Difference
If you work in health care IT, you have almost certainly heard "EHR" and "EMR" used interchangeably. Vendors do it. Clinicians do it. Even some of the trade publications do it. And in casual conversation, it usually does not matter. Everyone knows you are talking about the digital system where patient records live.
But if you are the person responsible for deploying, integrating, securing, or supporting that system, the distinction between an Electronic Medical Record (EMR) and an Electronic Health Record (EHR) is not just semantics. It has real implications for your architecture, your interoperability obligations, your compliance posture, and the regulatory frameworks your organization has to satisfy. Let's break down what the difference actually is, why it matters, and what it means for the people managing these systems on the ground.
The Short Version
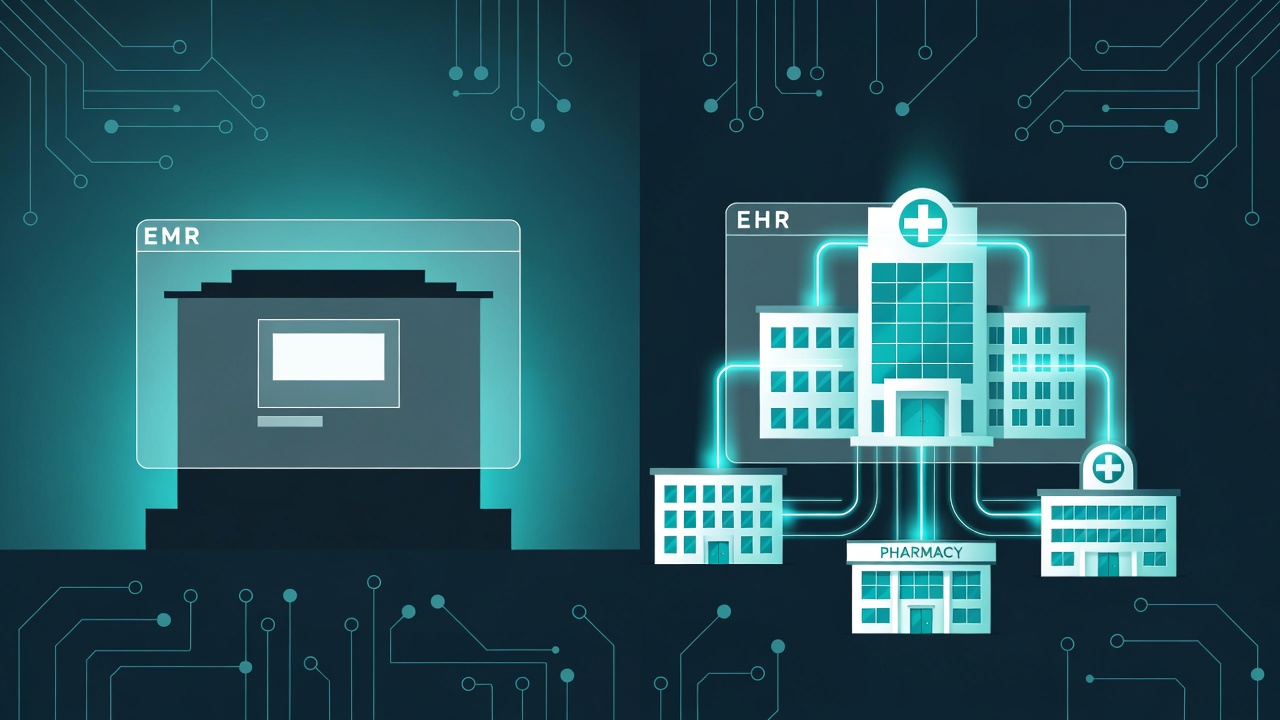
An EMR is a digital version of a paper chart. It lives inside one practice, one clinic, one facility. It stores patient demographics, visit notes, medication lists, lab results, and treatment history. It is purpose-built for documentation and internal workflow within that single organization.
An EHR does everything an EMR does, but it is designed to share data across organizations. It follows the patient across providers, facilities, specialists, labs, and pharmacies. It supports interoperability standards, connects to health information exchanges, and enables coordinated care across the continuum.
The Office of the National Coordinator for Health Information Technology (ONC) puts it this way: the EMR term came first, and early EMRs were truly "medical" - designed for clinicians to use within a single practice for diagnosis and treatment. EHRs go further by focusing on the total health of the patient across multiple care settings, designed from the ground up to be shared among authorized providers.
Think of it like this: an EMR is a filing cabinet. An EHR is a filing cabinet with a secure courier service built in.
Why This Matters for Health Care IT
For a solo IT administrator at a 25-bed Critical Access Hospital or a small physician practice, you might be thinking, "We have one system. Who cares what we call it?" Fair point. But understanding the distinction matters because federal programs, reimbursement incentives, interoperability mandates, and compliance obligations are all built around the EHR concept specifically.
Certification and Reimbursement
The federal government does not just encourage EHR adoption - it ties significant financial consequences to it. The CMS Promoting Interoperability Program requires eligible hospitals and providers to use Certified Electronic Health Record Technology (CEHRT) to avoid downward payment adjustments. For providers participating in the Merit-based Incentive Payment System (MIPS), failing to use CEHRT for the required reporting period can mean up to a 9% reduction in Medicare reimbursements.
That is not a small number. For a Critical Access Hospital operating on razor-thin margins, a payment adjustment like that can have serious budget implications.
CEHRT certification means the system meets specific technical standards established by ONC for interoperability, security, and data exchange. A basic EMR that does not support structured data sharing, FHIR-based APIs, or the US Core Data for Interoperability (USCDI) data elements will not qualify. If your organization is running a legacy system that functions as an EMR but lacks EHR-level capabilities, that is a conversation worth having with your vendor and your leadership.
Interoperability Is Not Optional Anymore
The health care industry spent years talking about interoperability as a goal. In 2026, it is an expectation - and increasingly, a legal requirement.
The 21st Century Cures Act, signed into law in 2016, established the prohibition on information blocking. This means that health care providers, health IT developers of certified health IT, and health information exchanges cannot engage in practices that interfere with the access, exchange, or use of electronic health information (EHI), unless an applicable exception is met.
This is not theoretical. Enforcement has been building since HHS directed increased resources toward information blocking in September 2025, and by February 2026, ASTP/ONC began issuing notices of potential nonconformity to certain EHR developers under the ONC Health IT Certification Program. The HHS announcement confirmed that these notices have gone out and continue to be issued. The HHS Office of Inspector General has the authority to impose civil monetary penalties of up to $1 million per violation for health IT developers and health information exchanges found to have committed information blocking. Health care providers face disincentives under CMS programs, including impacts to Medicare payments.
For IT teams, this means your systems need to support real data exchange, not just theoretical capability. If your EHR vendor claims FHIR API support but those APIs are not live, tested, and in use by authorized third parties, your organization could be exposed.
TEFCA: The National Network Is Growing
The Trusted Exchange Framework and Common Agreement (TEFCA) represents the federal government's push for a national-scale interoperability network. TEFCA went live in December 2023 when the first Qualified Health Information Networks (QHINs) were designated, and as of early 2026, the network has facilitated the exchange of nearly 500 million health records across more than 14,000 connected organizations representing over 79,000 unique connections to clinicians, hospitals, clinics, and other care facilities.
TEFCA standardizes the rules for who can exchange data, for what purposes, and under what conditions. It supports exchange for treatment, payment, health care operations, public health, individual access services, and government benefits determination (with the Social Security Administration recently joining the network).
For health care IT teams, TEFCA connectivity is increasingly becoming a baseline expectation rather than a nice-to-have. If your EHR vendor is not a TEFCA participant or subparticipant, or is not working toward that connectivity, that is worth a direct conversation. Ask your vendor specifically: Are you connected to a QHIN? Which exchange purposes do you support? What is your TEFCA roadmap?
The IT Infrastructure Behind the Distinction
From a technology perspective, the EMR-to-EHR distinction maps directly to how data moves through your environment.
Data Exchange Standards
EMR-style systems typically keep data inside a single facility. When information needs to go somewhere else, it often relies on faxing, PDF exports, or manual processes. If you have ever received a referral packet as a scanned PDF that arrived via a fax-to-email gateway, you know exactly what an EMR-level workflow looks like.
EHR systems are built for structured exchange using established standards. The key ones you need to know as a health care IT professional:
HL7 v2 remains the most widely deployed messaging standard in health care. It handles ADT (admit, discharge, transfer) messages, lab results, orders, and other transactional data. If you manage interface engines or integration platforms, you are almost certainly working with HL7 v2 messages today. Despite being decades old, it continues to be the workhorse of clinical system integration.
HL7 FHIR (Fast Healthcare Interoperability Resources) is the modern standard built on RESTful APIs, JSON, and web technologies. FHIR enables granular, resource-level data exchange - you can request a specific patient's medication list without pulling an entire document. It is the standard that ONC requires for certified health IT under the 21st Century Cures Act, and it powers patient access APIs, third-party app integrations, and the emerging TEFCA FHIR-based exchange.
C-CDA (Consolidated Clinical Document Architecture) is the document-based standard used for exchanging clinical summaries between systems. Continuity of Care Documents (CCDs) and discharge summaries are commonly exchanged using C-CDA formatting.
For quick reference:
| Standard | Primary Use Case | Why IT Teams Should Care |
|---|---|---|
| HL7 v2 | ADT messages, lab results, orders | Still dominant in legacy interfaces; you are likely already managing these |
| FHIR | API-based queries, patient access, app integrations | Required for CEHRT certification and TEFCA exchange |
| C-CDA | Clinical summaries, discharge documents, CCDs | Common format for transitions of care between organizations |
Quick reference: Key health data exchange standards for health care IT teams.
For IT teams at smaller organizations, you may not be building these interfaces yourself. But you need to understand what your EHR supports, what your interface engine handles, and where the gaps are. When a specialist's office calls and says they cannot pull your patient's records, or when a Health Information Exchange asks you to connect, knowing what standards your system actually supports (versus what it claims on a marketing sheet) is critical.
What This Looks Like in Practice
Consider a 25-bed Critical Access Hospital running an EHR with HL7 v2 interfaces to its lab system, pharmacy, and radiology. A patient is discharged and follows up with a cardiologist at a regional medical center 60 miles away.
In an EMR world, the hospital prints or faxes the discharge summary. It arrives as an unstructured document that the cardiologist's staff manually enters into their own system. The data is stale the moment it leaves the building, and there is no mechanism for the cardiologist to query back for updated information.
In an EHR world with proper interoperability, the discharge summary is available electronically through a health information exchange, a TEFCA-connected QHIN, or a direct secure messaging connection. The cardiologist's system can pull the most recent labs, medication list, and clinical notes in structured format. The data is current, searchable, and integrates directly into the receiving system's workflow.
That is the difference. And it is not just a clinical convenience - it is a patient safety issue, an operational efficiency issue, and a compliance issue.
HIPAA Considerations
Whether you are running an EMR or an EHR, the HIPAA Security Rule applies to all electronic protected health information (ePHI) your systems create, receive, maintain, or transmit. The Security Rule requirements under 45 CFR Part 164, Subpart C do not change based on what you call your system.
That said, an EHR's interoperability capabilities introduce additional security considerations that an isolated EMR does not:
Transmission security becomes more critical when data is flowing between organizations. Under 45 CFR 164.312(e)(1), covered entities must implement technical security measures to guard against unauthorized access to ePHI being transmitted over electronic communications networks. The encryption implementation specification under 45 CFR 164.312(e)(2)(ii) requires implementing a mechanism to encrypt ePHI whenever deemed appropriate. This is an Addressable specification, meaning the organization must implement it or document why an equivalent alternative measure is in place. It does not mean it is optional.
Access controls under 45 CFR 164.312(a)(1) require technical policies and procedures to allow access only to authorized persons or software programs. When your EHR exposes FHIR APIs or connects to external health information exchanges, the surface area for access control expands significantly. You need to verify that API access is properly authenticated, that third-party application authorization follows established protocols (like SMART on FHIR), and that audit logs capture who accessed what and when.
Audit controls under 45 CFR 164.312(b) require mechanisms to record and examine activity in information systems that contain or use ePHI. EHR interoperability means more systems and more actors touching patient data, which means your audit logging must account for external queries, API access, and data exchange transactions in addition to local user activity.
The bottom line: interoperability is a good thing, but it expands your security perimeter. As your EHR connects to more external systems, your security and compliance posture needs to keep pace.
Practical Guidance for Health Care IT Teams
So what should you actually do with this information?
Know what you have. Check the ONC Certified Health IT Product List to confirm whether your system holds current CEHRT certification. If it does not, understand the implications for your Promoting Interoperability reporting and Medicare reimbursement.
Ask your vendor hard questions. Do not accept "FHIR-ready" or "interoperability-capable" as answers. Ask: Which FHIR resources are currently live in production? Are your APIs tested and in use by third-party applications? Are you connected to a QHIN under TEFCA? What exchange purposes do you support? What is your roadmap for USCDI v3 compliance?
Understand your information blocking obligations. If you are a health care provider, you are an "actor" under the information blocking rules. That means you cannot unreasonably restrict patient or provider access to EHI. If your current system or processes prevent or discourage data exchange without meeting a recognized exception, you may be at risk. Review the information blocking exceptions under 45 CFR Part 171 and ensure your policies align.
Assess your interoperability posture. Document what interfaces you have, what standards they use, and what data actually flows. A FHIR API that exists but nobody uses is not interoperability - it is a checkbox. Map out where data gets stuck and where manual processes fill gaps that technology should handle.
Plan for TEFCA. Even if your organization is not directly connected to a QHIN today, your EHR vendor's TEFCA participation (or lack thereof) will increasingly affect your ability to exchange data efficiently. Understand where your vendor stands and factor TEFCA readiness into future procurement decisions. The network is scaling rapidly - revisit your vendor's TEFCA participation status at least quarterly, as connectivity details and supported exchange purposes are changing frequently.
The Bottom Line
The difference between an EMR and an EHR is not just a vocabulary exercise. It represents a fundamental shift in how patient data is created, managed, secured, and shared across the health care ecosystem.
For health care IT teams, the practical takeaway is this: isolated data is a liability. Federal regulations, reimbursement incentives, and the entire trajectory of health care interoperability policy are all pushing toward connected, standardized, auditable data exchange. Whether your organization is a large health system or a 10-provider rural clinic, understanding where your systems sit on the EMR-to-EHR spectrum - and what gaps need to be addressed - is essential to staying compliant, getting paid, and keeping patients safe.
The terminology might be confusing, but the direction is clear. Health care IT is moving toward interoperability, and your systems need to be moving with it.
This article is for informational purposes only and does not constitute legal or compliance advice. Covered entities and business associates should consult qualified legal counsel or compliance professionals before making decisions pertaining to HIPAA or IT infrastructure.
Sources
- Office of the National Coordinator for Health Information Technology (ONC), "EMR vs EHR - What is the Difference?" https://www.healthit.gov/buzz-blog/electronic-health-and-medical-records/emr-vs-ehr-difference
- CMS, "Certified EHR Technology" https://www.cms.gov/medicare/regulations-guidance/promoting-interoperability-programs/certified-ehr-technology
- ASTP/ONC, "Information Blocking" https://www.healthit.gov/topic/information-blocking
- HHS, "TEFCA, America's National Interoperability Network, Reaches Nearly 500 Million Health Records Exchanged" (February 2026) https://www.hhs.gov/press-room/tefca-americas-national-interoperability-network-reaches-nearly-500-million-health-records-exchanged.html
- The Sequoia Project (RCE), TEFCA Homepage https://rce.sequoiaproject.org/
- ASTP/ONC, "TEFCA" https://healthit.gov/policy/tefca/
- HL7 FHIR Specification https://www.hl7.org/fhir/overview.html
- ASTP/ONC, "Health Level 7 (HL7) Fast Healthcare Interoperability Resources (FHIR)" https://healthit.gov/interoperability/investments/fhir/
- HHS, "HHS Announces Crackdown on Health Data Blocking" (September 2025) https://www.hhs.gov/press-room/hhs-crackdown-health-data-blocking.html
- 45 CFR Part 164, Subpart C - Security Standards for the Protection of Electronic Protected Health Information https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-C/part-164
- ONC Health IT Dashboard, "Non-federal Acute Care Hospital Electronic Health Record Adoption" https://dashboard.healthit.gov/quickstats/pages/FIG-Hospital-EHR-Adoption.php
- Federal Register, "Health Data, Technology, and Interoperability: TEFCA" (December 2024) https://www.federalregister.gov/documents/2024/12/16/2024-29163/health-data-technology-and-interoperability-trusted-exchange-framework-and-common-agreement-tefca
- HHS Office of Inspector General, "Information Blocking" https://oig.hhs.gov/reports/featured/information-blocking/
- The Sequoia Project (RCE), TEFCA Frequently Asked Questions https://rce.sequoiaproject.org/rce/faqs/